

This division is put in place for the commissioned projects deriving from the Ministry of the Environment’s “Japan Environment and Children’s study (JECS)” and the currently undertaken research projects on “environments and health” with the funding from the Ministry of Education, Culture, Sports, Science and Technology, the Ministry of Health, Labour and Welfare, etc, to progress, and for new research projects to be developed.
Japan Environment and Children’s Study (JECS)
The Ministry of the Environment launched the “Japan Environment and Children’s study (JECS)” nationwide in January 2011. Its mission is to determine the effects of environmental factors on child health. Specifically, the study examines children’s exposure to chemicals (from the fetal to childhood stages) and living conditions so as to reveal the environmental factors’ effects on their health, and its research finding is to inform the creation of an appropriate risk management system against chemicals, etc.
The National Institute for Environmental Studies is the core center that oversees the study, and the core center is supported by the medical support center, which has been assumed by the National Center for Child Health and Development. Fifteen unit centers have been established across Japan through a recruitment process of open competition, and they work closely with the core center and the medical support center.
The subjects of the study are pregnant women residing in the geographical areas covered by the study, and cohort research (a type of research that follows up the same group over years) on 100,000 pregnant women, their children, and the children’s fathers nationwide is to be implemented. Recruitment of the subjects began in 2011, due to be finalized 3 years after. The children will continuously be followed up until they reach 13 years of age, and after all child subjects reach 13 years old, a 5-year period will be spent for data analysis, with the whole study to be concluded in 2032. The research consists of three sets of study, including full-scale studies that target all subjects of the research with the same survey items nationwide, detailed studies that target several thousand people randomly selected from the whole population 2 years after the beginning of subject recruitment, and follow-up studies that are designed and implemented by individual unit centers, etc. with their own budgeting, subject to the Ministry of the Environment’s approval.
Hokkaido Study on Environment and Children’s Health
The Hokkaido study on Environment and Children’s Health is an ongoing cohort study that began in 2002. The study consists of two prospective birth cohorts: the Sapporo (Toho hospital) cohort with one obstetric hospital in Sapporo City and the Hokkaido (large-scale) cohort with 37 hospitals and clinics in the Hokkaido prefecture. Hokkaido is the northern most prefectures and the second largest island of Japan; it has an area of 83,457 km2 (Figure 1).
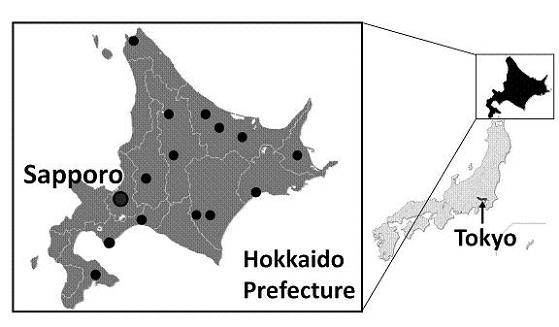
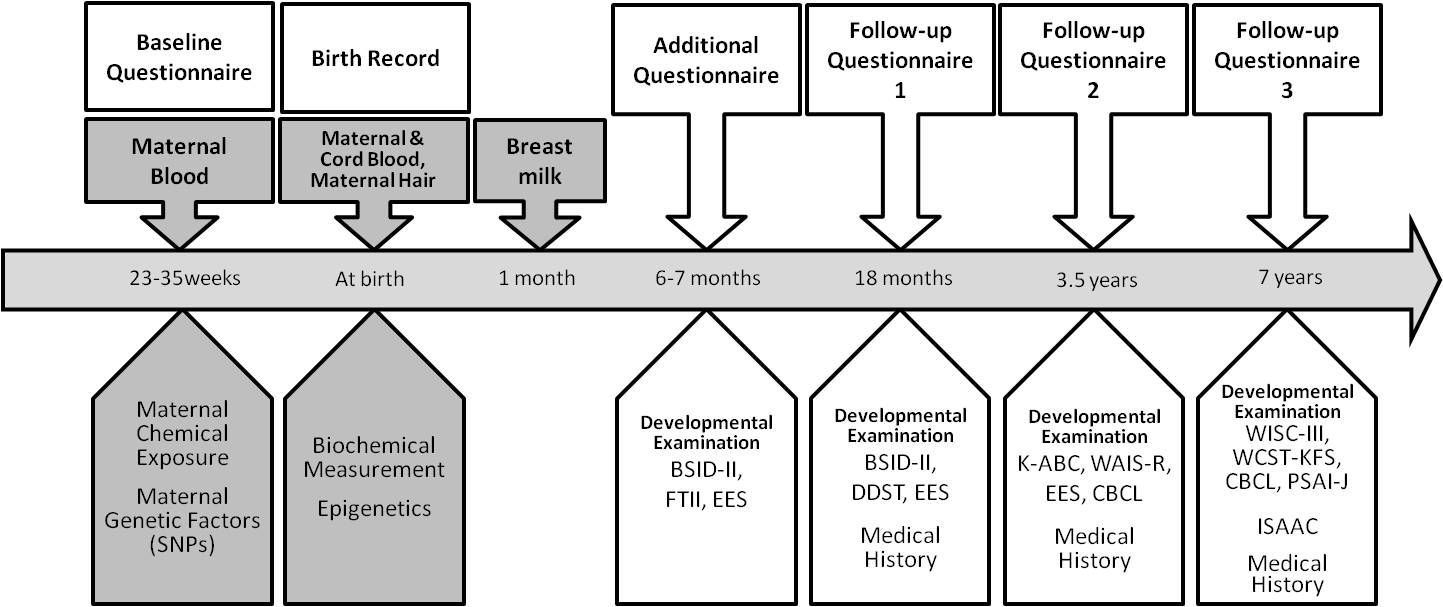
The large circled dot indicates Sapporo city (the prefectural capital of Hokkaido). The block dots indicate the geographical distributions of the collaborating hospitals and clinics outside of Sapporo city. The enrollment of the Sapporo cohort (Toho hospital) was conducted from July 2002 to October 2005. The subjects were women that were enrolled at 23-35 weeks of gestation and delivered at the Toho hospital. All of the subjects were residents of Sapporo City or surrounding areas. In the Sapporo cohort, observations were focused on the association between child growth, neurodevelopment, allergy and infectious diseases, and low-level exposure to environmental chemicals during pregnancy and infancy (Figure 2).
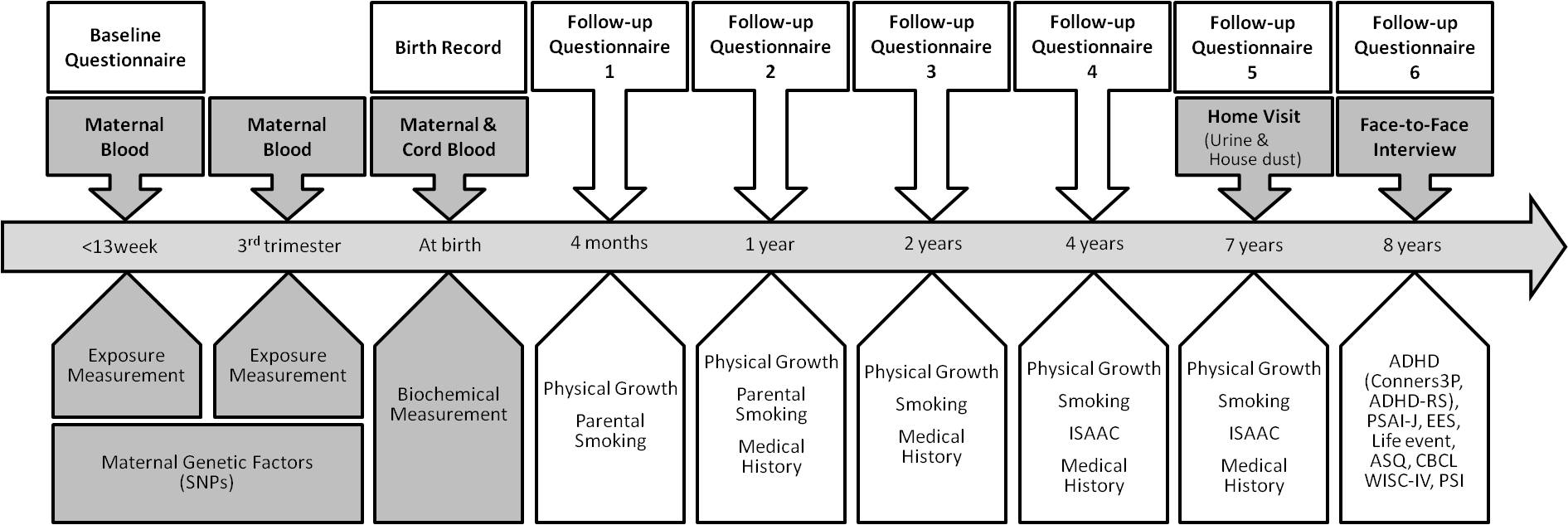
Since February 2003, the Hokkaido (large-scale) cohort has continued to enroll women during early pregnancy (<13 weeks of gestational age) that visited one of associated hospitals or clinics in the study area for prenatal health care in the maternity unit. This cohort consists of 20,940 pregnant women as of March 2013. In total, 37 hospitals and clinics in the Hokkaido prefecture participated in the study. The Hokkaido cohort (Figure 3) was established to assess the prevalence of congenital anomalies including cleft lip and palate, congenital heart defects, hypospadias and cryptorchidism. In addition, this cohort was used to explore the possible causes of these malformations, as well as the prevalence of childhood allergies and neurodevelopmental disorders including attention deficit hyperactivity disorder (ADHD).
For the last ten years, we followed pregnant women and their offspring, measuring various environmental chemicals. The levels of 29 congeners of dioxins and dioxin-like PCBs (7 PCDDs, 10 PCDFs, 4 Non-ortho PCBs, and 8 Mono-ortho PCBs ), 58 congeners of the other PCBs, and 5 congeners of OH-PCBs in maternal blood and breast milk were measured using a high-resolution gas chromatography/high-resolution mass spectrometer (HRGC/HRMS) at the Fukuoka Institute of Health and Environmental Sciences. Eleven perfluoroalkyl acids (PFAAs) of PFCs [perfluorohexanoic acid (PFHxA), perfluoroheptanoic acid (PFHpA), perfluorooctanoic acid (PFOA), perfluorononanoic acid (PFNA), perfluorodecanoic acid (PFDA), perfluoroundecanoic acid (PFUnDA), perfluorododecanoic acid (PFDoDA), perfluorotridecanoic acid (PFTrDA), perfluorotetradecanoic acid (PFTeDA), perfluorohexane acid (PFHxS) and perfluorooctane sulfonate (PFOS)] were measured in maternal plasma using simultaneous analysis with liquid chromatography-tandem mass spectrometry (LC/MS/MS) and ultraperformance liquid chromatography in combination with triple quadrupole mass spectrometry (UPLC-MS/MS) at the Hoshi University, as well as Research Faculty of Agriculture, Hokkaido University. The levels of persistent organochlorine pesticides in maternal blood were analyzed by a GC/negative-ion chemical-ionization mass spectrometry (GC/NCIMS) and a GC/high-resolution mass spectrometry (GC/HRMS) at IDEA Consultants, Inc. Total mercury levels in maternal hair samples were measured by an oxygen combustion-gold amalgamation method using an atomic absorption detector at the National Institute for Minamata Disease. To determine maternal phthalate exposure levels, MEHP (a metabolite of DEHP) levels in maternal blood were analyzed by GC/MS at Nagoya University. Bisphenol A concentrations in maternal and cord blood were analyzed by isotope dilution LC-MS/MS (ID-LC-MS/MS) at IDEA Consultants, Inc. Cotinine concentrations in maternal serum were measured using an enzyme-linked immunosorbent assay (ELISA) kit to evaluate smoking exposure levels. In the Sapporo cohort, with the purpose of assessing the neurodevelopment of the children, several behavioral examinations were conducted during each study period. The Bayley Scales of Infant Development second edition (BSID-II), the Fagan Test of Infant Intelligence (FTII), the Japanese version of the Denver Developmental Screening Tests (DDST), the Kaufman Assessment Battery for Children (K-ABC), and the Wechsler Adult Intelligence Scale-Revised (WAIS-R), the Wechsler Intelligence Scale for Children third edition (WISC-III) and the Wisconsin Card Sorting Test (WCST-KFS version), the Evaluation of Environmental Stimulation (EES), the Japanese version of the Child Behavior Checklist (CBCL), Pre-School Activity Inventory-Japanese version (PSAI-J) were used. In addition, we also obtained the children’s medical history of atopic dermatitis, asthma, allergies, otitis media, pneumonia or bronchitis and chickenpox. Genes that were analyzed using the SNP assay. The polymorphisms of CYP1A1 (cytochrome P450, family 1, subfamily A polypeptide 1), CYP1A2 (CYP1 subfamily A polypeptide 2), CYP1B1 (CYP1 subfamily B polypeptide 1), AHR (aryl hydrocarbon receptor), AHRR (AHR repressor), NQO1 (NAD(P)H: quinone oxidoreductase 1), CYP2E1 (CYP2 subfamily E polypeptide 1), and MTHFR (methylenetetrahydrofolate reductase) were analyzed. In addition, copy number variations (CNVs) in GSTM1 (glutathione S-transferase mu-1) and GSTT1 (glutathione S-transferase theta-1) were also evaluated. The design of our study is a prospective cohort study intended to collect data on environmental exposures during fetal development and to control for potential confounders. The detailed measurements are adequate to detect the various effects of perinatal environmental and genetic determinants on childhood outcomes. In the Sapporo cohort study, face-to-face examinations for neurodevelopment assessment were conducted. The Hokkaido cohort had been the largest birth cohort in Japan until 2011 when the nation-wide cohort study, the Japan Environment and Children’s Study (JECS), was launched based upon our study design. Moreover, there has been an avid movement toward collaborating and integrating existing birth cohort studies across borders. The primary purpose of these birth cohort consortiums are to obtain evidence-based results by using data from larger sample sizes (meta-analysis), as well as obtaining more applicable and generalizable results by integrating data beyond regions, countries and ethnicities. In Asia, the Birth Cohort Consortium of Asia (BiCCA) is now calling for participation to all existing Asian birth cohorts. [http://www.bicca.org]. Although there are many challenges associated with coordinating different cohort studies, we do believe that it is a worthy endeavor. This study was funded by a Grant-in-Aid for Scientific Research from the Japanese Ministry of Health, Labor and Welfare, the Ministry of Education, Culture, Sports, Science and Technology and the Japan Society for the Promotion of Science and Ministry of Environment. We would like to express our appreciation to all of the study participants of The Hokkaido Study on Environment and Children’s Health. We express our profound gratitude to all personnel in the hospitals and clinics that collaborated with the study: Sapporo Toho Hospital, Keiai Hospital, Endo Kikyo Maternity Clinic, Shiroishi Hospital, Memuro Municipal Hospital, Aoba Ladies Clinic, Obihiro-Kyokai Hospital, Akiyama Memorial Hospital, Sapporo Medical University Hospital, Hokkaido University Hospital, Kitami Red Cross Hospital, Hoyukai Sapporo Hospital, Gorinbashi Hospital, Hashimoto Clinic, Asahikawa Medical College Hospital, Hakodate Central General Hospital, Ohji General Hospital, Nakashibetsu Municipal Hospital, Sapporo Tokushukai Hospital, Asahikawa Red Cross Hospital, Wakkanai City Hospital, Kushiro Rosai Hospital, Sapporo-Kosei General Hospital, Shibetsu City General Hospital, Nikko Memorial Hospital, Sapporo City General Hospital, Kohnan Hospital, Hakodate City Hospital, Hokkaido Monbetsu Hospital, Tenshi Hospital, Hakodate Goryoukaku Hospital, Nakamura Hospital, Kin-ikyo Sapporo Hospital, Kitami Lady’s Clinic, Engaru-Kosei General Hospital, Kushiro Red Cross Hospital, Nayoro City General Hospital and Obihiro-Kosei General Hospital.
Indoor air quality and Health
The airtightness of buildings has been increasing in Europian countries since the 1970s. This has resulted in an increase in health problems caused by poor indoor air quality (IAQ) termed sick building syndrome (SBS). In the 1990s, some Japanese people living in newly built or renovated houses reported a variety of nonspecific subjective symptoms resembling SBS, which was designated sick house syndrome (SHS). Since SHS patients dwell in new or renovated houses, indoor chemicals emitted from building materials, including formaldehyde and volatile organic compounds (VOCs), are acknowledged as the major sources of SHS in Japan. However, this Japanese concept of SHS lacks many other factors such as biological, physical, and psychosocial factors as well as dampness problems. Therefore, since SBS/SHS problems contribute to IAQ, we are continuing to conduct epidemiological studies in homes involving both environmental monitoring and questionnaires.
Table 1 summarizes each epidemiological study.
Table 1: Summary of the 4 studies

The first study began in April 2001. Using the list of single-family dwellings constructed by 24 housing companies in Sapporo, we distributed questionnaires to 564 occupants and subsequently conducted environmental measurements in 96 dwellings. The concentrations of aldehydes and VOCs in the air were measured. Viable airborne fugal species were determined, and floor dust was collected to measure dust mite allergens. Dampness signs were inquired about in a questionnaire.
In 2003, we organized a study group from 6 different regions in Japan to initiate the second study (Figure 1).

Surveys were conducted according to the same protocol in all regions. The questionnaires were distributed to the occupants of 6,080 dwellings built within the last 7 years from a list of approved building plan applications. There were a total of 2,297 respondents. The first environmental measurements were conducted in 425 dwellings in 2004, and all inhabitants filled in health questionnaires including questions about SHS and allergies. The international standardized questionnaire for SBS, the MM questionnaire, was used to determine SHS. Follow-up measurements were conducted twice in 2005 and 2006. In addition to measuring aldehydes, VOCs, fungi, and mite allergens, semi-volatile organic compounds (SVOCs including 7 phthalates, 11 phosphorus flame retardants [PFRs], 16 pyrethroids, and organophosphate pesticides in the air and dust) and microbial VOCs (MVOCs) were measured in 2006. The research group published a book based on these studies in 2009 titled, Manuals of Sick House Syndrome: Consulting and Countermeasures (ISBN978-4-8192-0215-2).
In the first 2 studies, the prevalence rate of SHS was higher among children than among adults. Thus, the third study focused on elementary school children. We approached public schools in each region for cooperation. A total of 10,816 questionnaires were distributed; the response rate was 71%. Like previous studies, environmental measurements were conducted in 178 homes over the following 2 years. This study differed in that we included not only newly built single-family dwellings, but also multi-family apartments and old single-family dwellings. In this study, we also collected urine samples from all family members for biological monitoring.
Since 2011, we have been conducting an IAQ study on 7-year-old children participating in the Hokkaido Study on Environment and Children’s Health. This fourth study is targeting asthma and allergies as primary health outcomes. In parallel to investigators’ home visits for environmental measurements, we ask each participant to collect dust and urine samples. This challenge enables sample collection throughout the Hokkaido area (83,457 km2). In addition, the prospective cohort study design will eliminate recall bias as a potential confounder.
We hope our research provides scientific evidence to improve IAQ and thus people’s health. In addition, we intend to continue our research projects in related fields.
We would like to acknowledge that these studies are financially supported by a Health Science Research Grant for Research on Environmental Health from the Ministry of Health, Labour, and Welfare of Japan and by the Environment Research and Technology Development Fund of the Ministry of the Environment, Japan. We thank all the study participants and are grateful to all of our colleagues.
Support networks for the elderly
Introduction of the elderly care public insurance system sees the ongoing development of infrastructure to support elderly people’s health and livelihood in their community. Adding to the enhancement of support provided by specialized agencies and public authorities, it is important to expand practical and emotional support networks for the elderly, taking into account that their immediate relationships, such as family, friends, and neighbors, impact their mind and body.
Our research group on support network for the elderly has carried out long-term prospective cohort studies since 1991 in three regions in Hokkaido (a large city, a rural village, and a depopulated former coal mining district) and examined from multiple perspectives the links between elderly support networks and various health indicators such as ADL, depressiveness, premature death, requirement for care, and medical expense.
Through analyses of support networks in terms of regional difference, gender difference, and age difference, it has been revealed that males living alone in large city and the old-old (especially women) would require a stronger support, that males lower their risk of premature death by taking part in a group or by receiving emotional support, and that females lower their future risk of slipping into a care-requiring condition when they have intimate relationships with their neighborhood or when they are in a position of supporting others, etc.
We also conducted intervention research with preventive home visits targeted at elderly people living in their own home, in Honbetsu Town and Takasu Town in 2007 and in Hidaka Town and Shinhidaka Town in 2008. The result indicated that a home visit that involves the use of tools in occupational therapy has preventive effects on cognitive function and depressive symptoms.